Plastic Surgery
After You've Lost the Weight
A roadmap and user’s guide to what to do after the weight comes off. A personal approach.
Introduction
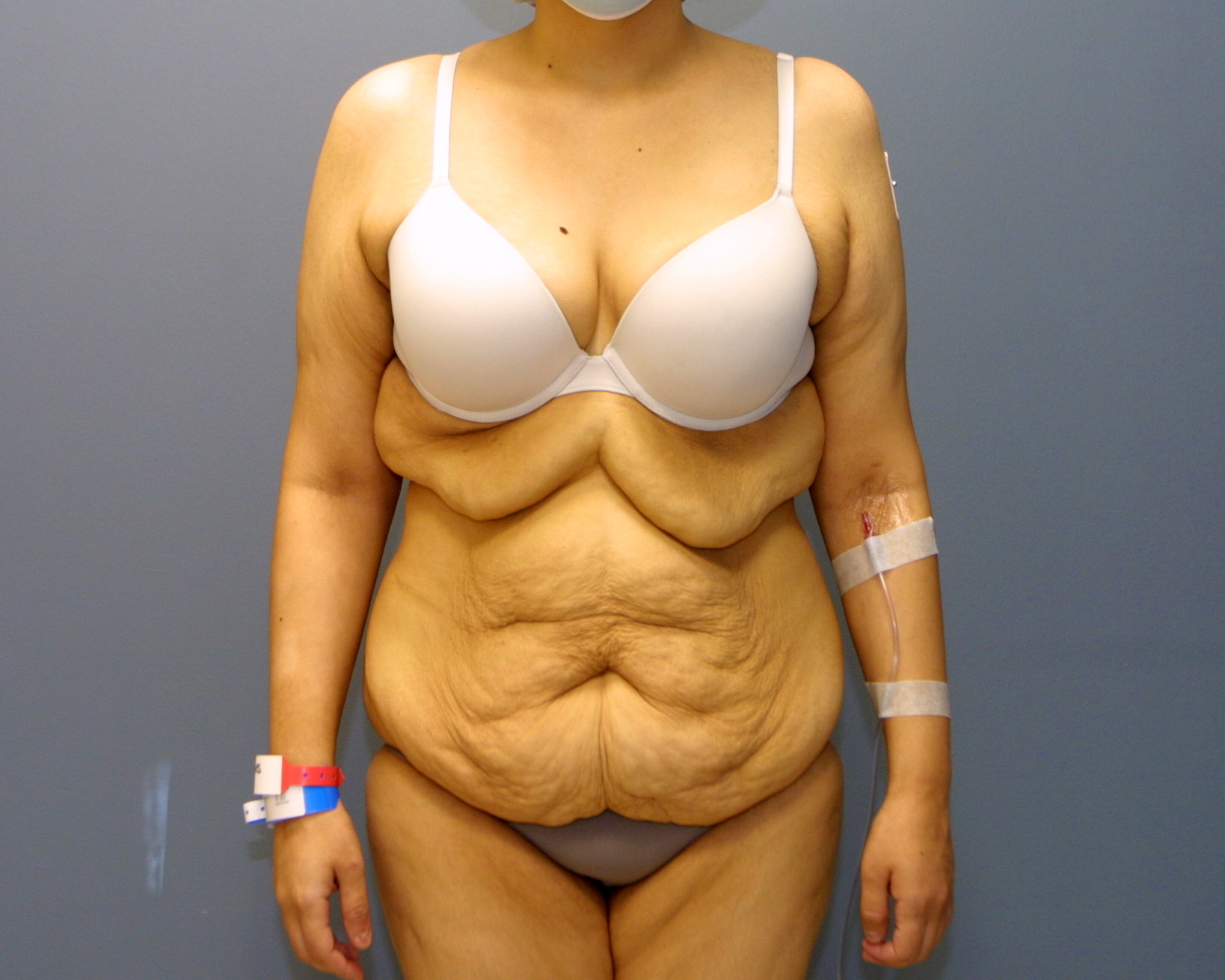
What a difference a day (or two) can make.
This patient has lost over 100 pounds and has had an upper body lift and a Fleur-de-Lis tummy tuck.
{kind=link}
{kind=link}
After diet, exercise, and maybe getting some help from the latest weight loss drugs, you are now facing droopy skin in areas you’ve never imagined. I call this “the punishment for doing everything right.” Once you’ve gotten there the path to choosing the correct operations can be confusing. This is a one-page site that covers options in skin tightening from top to bottom. It is about the surgical options, but not all the surgical details. Those can be found at my other sites. This site reflects my personal experience, and how I have guided my massive weight loss patients for over two decades. My way is, of course, not the only way but as you read on, I hope you enjoy and find common sense in my approach. You can read from top to bottom or use the links to jump around as you wish.
Click on the link to each topic below or scroll down


Diet & Exercise:
Without question, the safest way to lose weight also happens to be the most difficult, most unpleasant, and most prolonged. This would be diet and exercise. Medical Fact: If you burn more calories than you take in, your weight will come off. It requires a will of steel and strict behavior modification. Kudos to you if you can do this, because it is the safest, healthiest, and most long-lasting. For this method, I tend to see two failure points. Self deception, eating more than you really should and, oddly enough, over-exercising. With stalwart enthusiasm people will get that New Year’s resolution gym membership and do too much too soon and actually injure or slow themselves down. Be kind to your body. Increase exercise gradually. It becomes easier as the weight begins to come down. With respect to self deception, count your calories honestly. All it takes is one misstep – one cocktail or bag of chips – to tip the weight loss scales. I am a big fan of Jenny Craig or Nutrisystem to help you stay on track. If you are honest with their calorie counting apps, you WILL lose weight.
Surgical Weight Loss:
Surgical weight loss definitely works, but I suspect will be less common because of the success of the drug options that I will discuss below. Surgical weight loss is not perfect. It has risks, recovery, failure points and did I say risks? If you fail with other modalities the risk may be worth it, but if you can accomplish the weight loss without it I think you are better off.
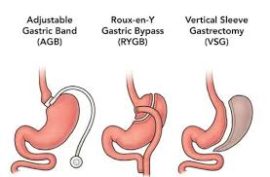
I personally think that intestinal bypass works best, but it can have long term metabolic consequences.
Gastric bypass, lap band and others that restrict input (rather than bypass nutrition) work, but also require strong patient participation. High calorie liquids are the biggest failure points and go right through these restrictions.
Weight Loss Drugs:
It’s hard to keep them all straight, but GLP-1 drugs (Ozempic, Zepbound, etc.), which were originally developed to help blood sugar control in diabetics, are all the rage now. I don’t tend to jump on bandwagons, but I have seen some remarkable transformations using these drugs. Simplistically, they make your brain feel less hungry and your stomach feel more full at the same time.
I have two concerns about these drugs:
1) It’s the wild west out there. These drugs are showing up in value packs, Groupons and internet ads. While at present I believe that they are safe and effective, be sure you are seeing a real doctor and being monitored appropriately. Liver tests and other parameters must be watched. Be sure your doctor is sourcing these drugs correctly and that you are getting what is prescribed. Be careful.
2) While getting on these drugs is easy, getting off may be harder. Roadmaps for stopping vary — I don’t think it’s all worked out yet.
3) When in doubt, see the diet and exercise section above.
General concepts for the weight loss patient
These are the things I want all of my massive weight loss patients to know prior to their surgery.
Skin Relaxation: Weight loss patients tend to see more skin relaxation than others after surgery. The average postpartum mom who’s weight may go up-and-down 20 to 40 pounds will usually still have pretty good skin elasticity. After massive weight loss, the once overstretched skin loses some inherent elasticity and may relax more after surgery. This is not a bad thing, but worthy of knowing to give realistic postoperative expectations.
Bleeding: When the body gets bigger, the blood vessels increase in size to provide adequate blood supply. While the fat diminishes with weight loss, the vessels still stay big. While postoperative bleeding is rare, great care is taken to avoid it in all patients, let alone the weight loss patients.
You Can’t Do Everything at Once: There is indeed such a thing as too much surgery in one day and safety must come first. In my own practice, I recommend surgeries that we can accomplish safely in single outpatient setting. Usually, this is one or two procedures, and on rare occasions, more. With a good helper at your disposal, I feel that you are much better off recovering in your own home than in a hospital. Sadly, hospitals harbor ill patients and bacteria. No one sick lives in my outpatient facility.
Other Things You Will Notice: Massive weight loss patients are often considered to be “works in progress” as there is always something to tighten. When one area looks better, patients then tend to notice other areas. I try to preview these areas with my patients so that they know what to expect before they start their initial surgeries. Even more importantly, I try to provide a surgical plan so that one surgery will not preclude another in the future.
Before I dive into the surgeries there are some basic principles I want you to know about.
Be at the weight you want to be before surgery: If you have a beautiful tummy tuck or breast lift and lose another 30 pounds, you may need another tummy tuck or breast lift. It’s worth waiting to get to your target, realistic goal weight. Make your goal a healthy weight but don’t aim to be skeletally thin. When tissues are too thin, the surgical risks can increase. When in doubt seek my guidance.
Do not starve yourself until the day before your surgery: You must have good nutrition to heal uneventfully after surgery. Your body must not be eating itself while it is trying to heal. I recommend a stable weight with good protein and nutrition 4-6 weeks prior to your procedure. You don’t have to gain weight, just be stable.
Be under medical supervision: Address any medical issues ahead of time. Sleep apnea, diabetes, and high blood pressure must all be in control prior to surgery. You may need a stress test or sleep study. Look into these things ahead of time or they will delay your planned surgeries. Some of these studies can be very difficult to schedule.
Stop all weight loss medications at least two weeks before your surgery: Some can lead to blood pressure problems and some can lead to pulmonary issues in surgery. Be sure you relay everything that you take orally. Many supplements can lead to problems with anesthesia or bleeding.
You can’t do this alone!: Have a friend, partner, or family member with you to help with recovery. You need to be taken home and attended to. You don’t need a health care professional, just someone who cares.
Weight loss can lead to deflation of facial fat. While that may sound good, when the face deflates, it can lead to sagging of the jowls, deeper facial lines, and most visibly, laxity in the neck. While there may be some role for facial fillers, they won’t do much if the skin is loose. The option that tends to stay and help solve this issue is a facelift, sometimes combined with an eyelid lift if they are saggy as well.
Skin tightening alone does not tend to hold up well over time. I favor tightening of the underlying muscles as well. While some physicians will elevate the muscles I tend to pull them together using sutures. This is called plication and in my opinion, has a lower risk of facial nerve injuries.
As touched on in the General Concepts section above, weight loss patient skin tends to relax more because of poor skin elasticity. Interestingly, second facelifts down the road may stay tighter and hold up longer because the first facelift sets up scaffolding of scar tissue under the skin that leads to a stronger pull.
Facelift and Upper Eyelids
{kind=link}
{kind=link}




Neck Tightening
Breast
The above options are discussed more fully in my www.DCBreast.com site. On this site I want to put these into context with the massive weight loss patient.
Augmentation: Despite massive deflation of the breast fat, some weight loss patients are actually not too droopy. In other words, they may not need a lift. For the right patient, an implant alone may be all that is needed. It depends on how much tissue hangs below the bottom of the breast and the size of the implants chosen. All patients look a little bit scary after augmentation surgery until the muscles relax and the implants fill out the breasts. Because of increased skin laxity the weight loss patient may look scarier. In some patients with a moderate degree of droop it is not always clear if a lift will be needed. On many occasions my patients will allow me to use my discretion and decide about a lift in the operating room after the implants are placed. The paitent below has some laxity and is bordering on the need for a lift. A high profile breast implant was able to fill out the loose skin.
{kind=link}
{kind=link}
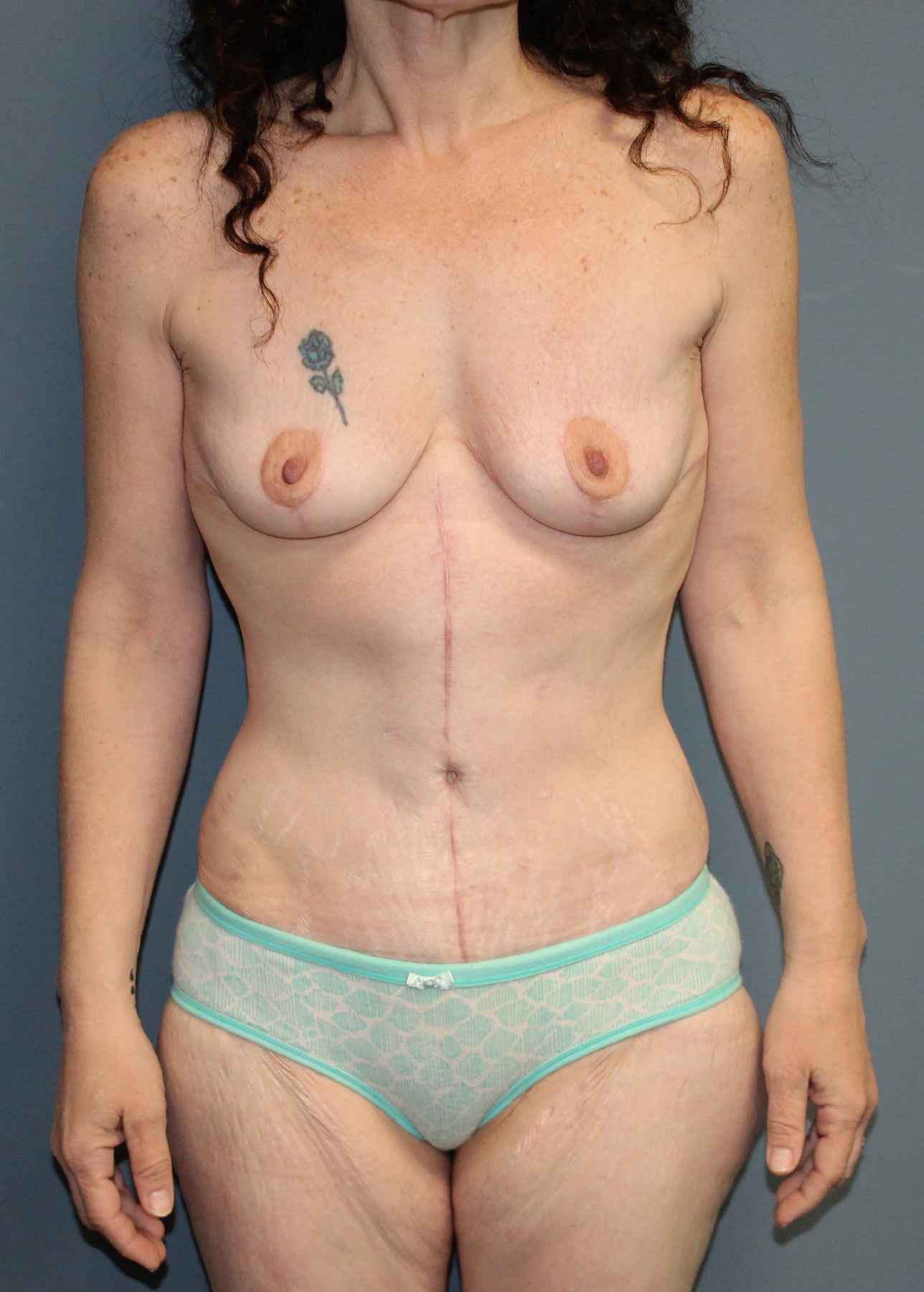
Breast Lift Alone: Many weight loss patients have sagging breasts. A mastopexy, or breast lift, simply tightens the skin of the breast. Think of it like removing the fabric from a bra that is too loose. Many patients think that a breast lift will make them look like they have breast implants. That is not the case. Implanted breasts have a bulge up top. Natural breasts, even lifted or tightened, will take on a teardrop shape and regain some droop. I think some droop is a good thing and makes a result more believable. The heavier the breast, the more it will relax, and weight loss patients tend to relax more than others. For a patient with a very heavy breast I might suggest lightening the load with at least some degree of breast reduction.
Breast Lift (No Implants) in Weight Loss Patients Who Also had Fleur-de-Lis Tummy Tuck
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Breast Lift With Augmentation: Breast lift with augmentation is discussed more fully at www.dcbreast/implants with lift. It is one of the more variable surgeries in the U.S. with a higher touch-up rate because implants, which need to drop, and lifts, which we want to stay tight, fight one another after surgery. This variability is increased in the massive weight loss patient due to poor skin tone. A weight loss patient might retighten a lift sooner than the average patient. In some of my patients with this combination, I will augment with an implant but also do a limited reduction. Too much reduction over an implant can stress blood supply and the healing breast. This limited reduction while augmenting is an effort to get rid of some of the natural tissue that wants to go south after surgery.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
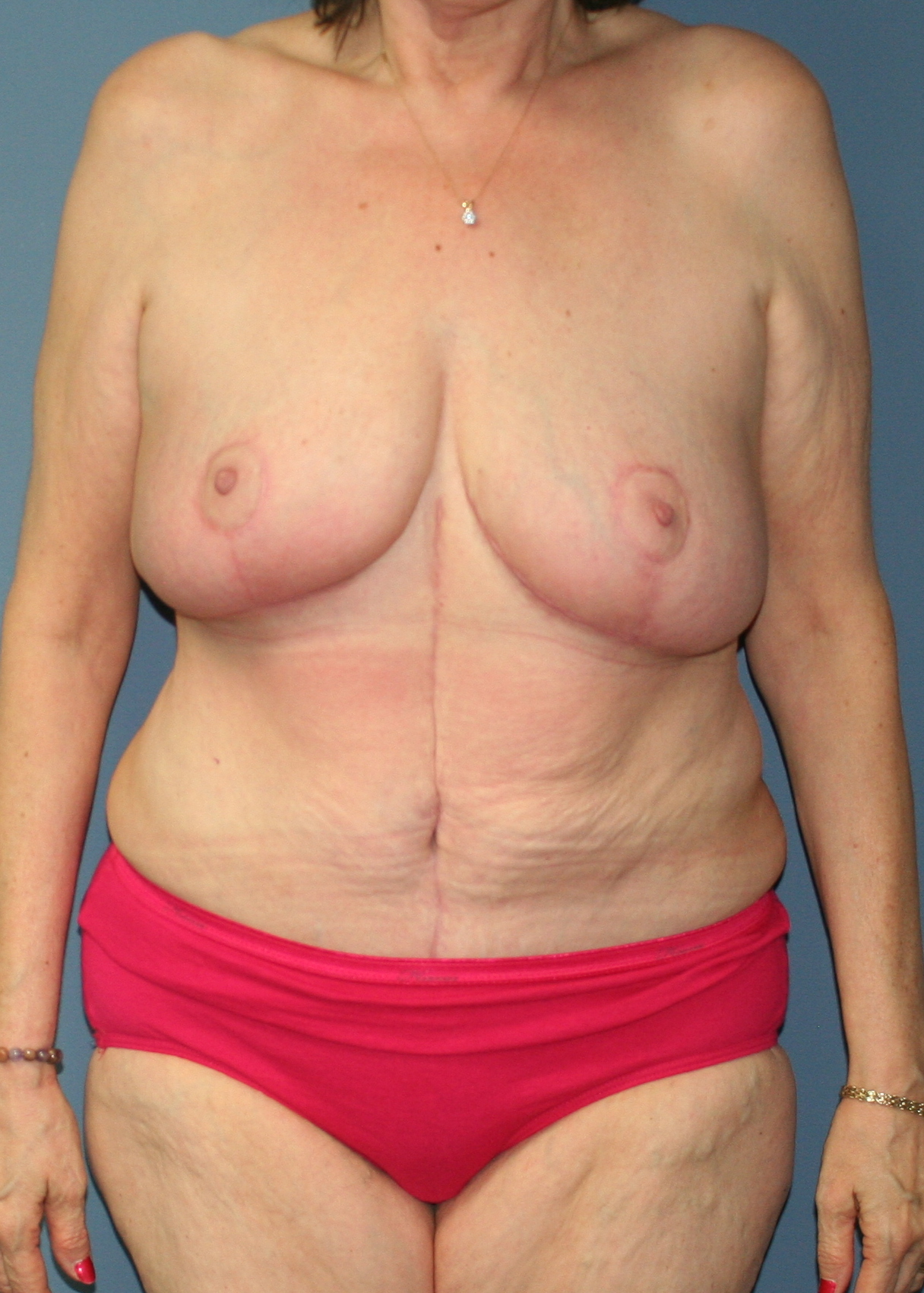
Breast Reduction: Like a lift, the reduced breast may relax more than average in the weight loss patient due to skin tone. I find the degree of droop very much related to the size of the breasts we leave behind. Lighter will stay higher, heavier will go south more. In an effort to add support, some surgeons will add an absorbable mesh in the breast. I hesitate to add foreign materials which run the risk of infection or extrusion.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Arm Lift/Brachioplasty
What is a Zone 4 Brachioplasty?
Weight loss patients are prone to laxity, particularly of the upper arm. Many will come to see me for liposuction, but that is not the answer. If skin is loose, then removing more fat will make the arms more lax. Losing a hundred pounds of weight or more, these patients have done their own liposuction and that is why they are loose in the first place. They need skin tightening. The diagram below is from plasticsurgerykey.com. It shows the four zones of the arm when considering brachioplasty. Most non-massive weight loss brachioplasty happens in zone 2 and 3, tightening the skin up the arm and into the armpit. Massive weight loss patients often have laxity in zone 4 as well, extending down the chest wall. So, a zone four brachioplasty is much more common in the weight loss patient.
Whichever brachioplasty I might recommend, you have to really want this surgery. Brachioplasty can lead to wider and sometimes thicker scars because of the motion of the arm.
Important Note: If I have a patient that wants a breast lift or a reduction, as well as a zone 4 brachioplasty, I prefer them to have the breast lift or reduction first, heal and then complete the brachioplasty later. When we elevate the upper breast skin for a reduction or lift, the outer sides of the breast gets its blood supply from the shoulder and sides of the chest. If the patient has a long incision there from a zone 4 brachioplasty, I am concerned about blood supply to that skin. Once the breast has healed, it will not affect the blood supply to the brachioplasty.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}

Abdomen - tummy tuck
A tummy tuck after weight loss is perhaps the most gratifying surgery and most often the first. I think of it as the gateway surgery after massive weight loss. Most patients only have heard of a mini tummy tuck or a full tummy tuck, but in the weight loss community they must also be taught about the Fleur-de-Lis tummy tuck.
Mini Tummy Tuck
Most tummy tucks pull loose skin downward. The more you can pull down, the more excess skin you can get rid of. If you have a short scar, you can only take a few inches of vertical tightening. That would be a mini tummy tuck and it is useless to the massive weight loss patient. Below is a mini tummy tuck helping to level out a c-section scar skin overhang. Most weight loss patients have far more laxity than this.
{kind=link}
{kind=link}
Full or Extended Tummy Tuck
While I will sometimes see a good candidate for a mini tummy tuck, I would consider most of my tummy tucks extended. Not all scars are the same length. I think of them as extended because I bring the scar out as needed to remove as much extra skin as possible. Remember, the more we pull down, the more we need to go out to the sides. Each patient is different. If the scar does not go far enough to the sides, a fold of skin known as a “dog ear” will remain.
{kind=link}
{kind=link}
{kind=link}
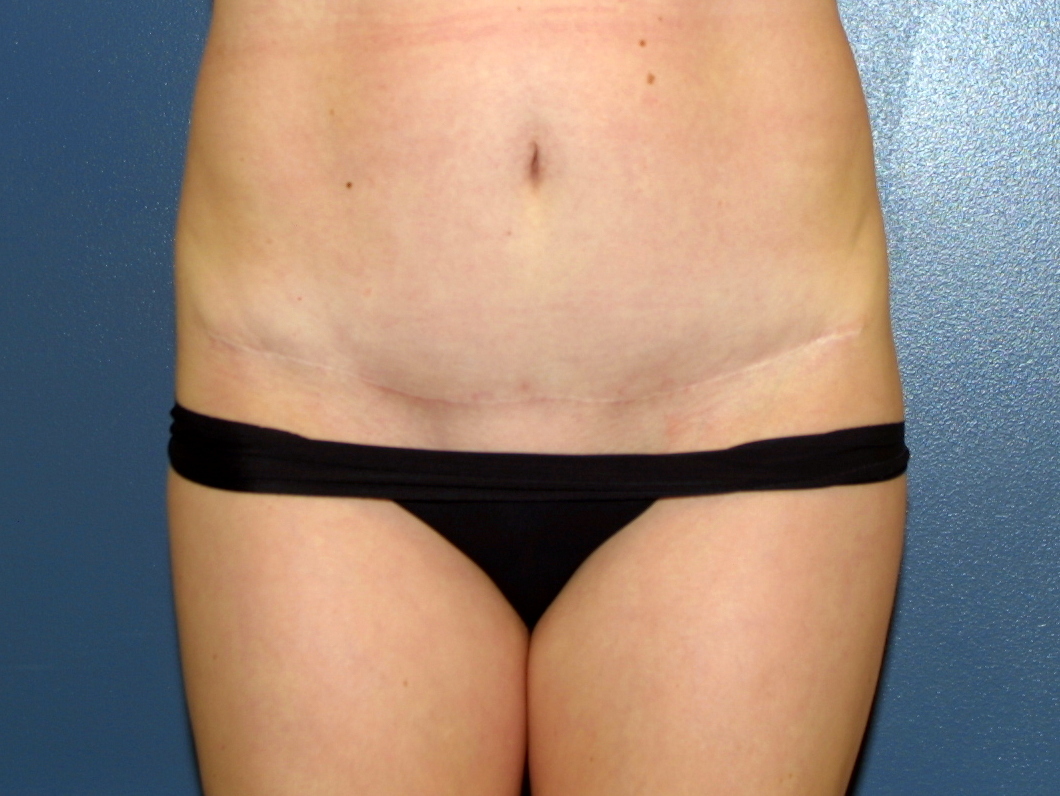
Fleur-de-Lis Tummy Tuck
In any patient, but particularly in the massive weight loss patient, skin is not just loose top to bottom, but side to side as well. A Fleur-de-Lis tummy tuck takes a vertical wedge right out of the middle of the abdomen, giving a side to side pull in addition to a top to bottom pull. This tuck leaves a scar down the middle of the abdomen. Some will not want to have that scar, which is fine, they will just continue to have more side to side laxity, which is also fine as long as the patient is prepared and understands why.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Important Note: If a massive weight loss patient has horizontal laxity, but does not want a Fleur-de-Lis tummy tuck then I use my judgment about the degree of muscle tightening we will do. When we repair muscle separation in a tummy tuck (diastasis), bringing the muscles together pulls the skin side to side in with it. In the non-massive weight loss patient, the skin has enough elasticity to be laid out smoothly. In the massive weight loss patient this may lead to a big lump of excess skin in the middle.
If I am performing a Fleur-de-Lis tummy tuck, I tighten muscles as I normally would because I can remove the extra midline excess skin.
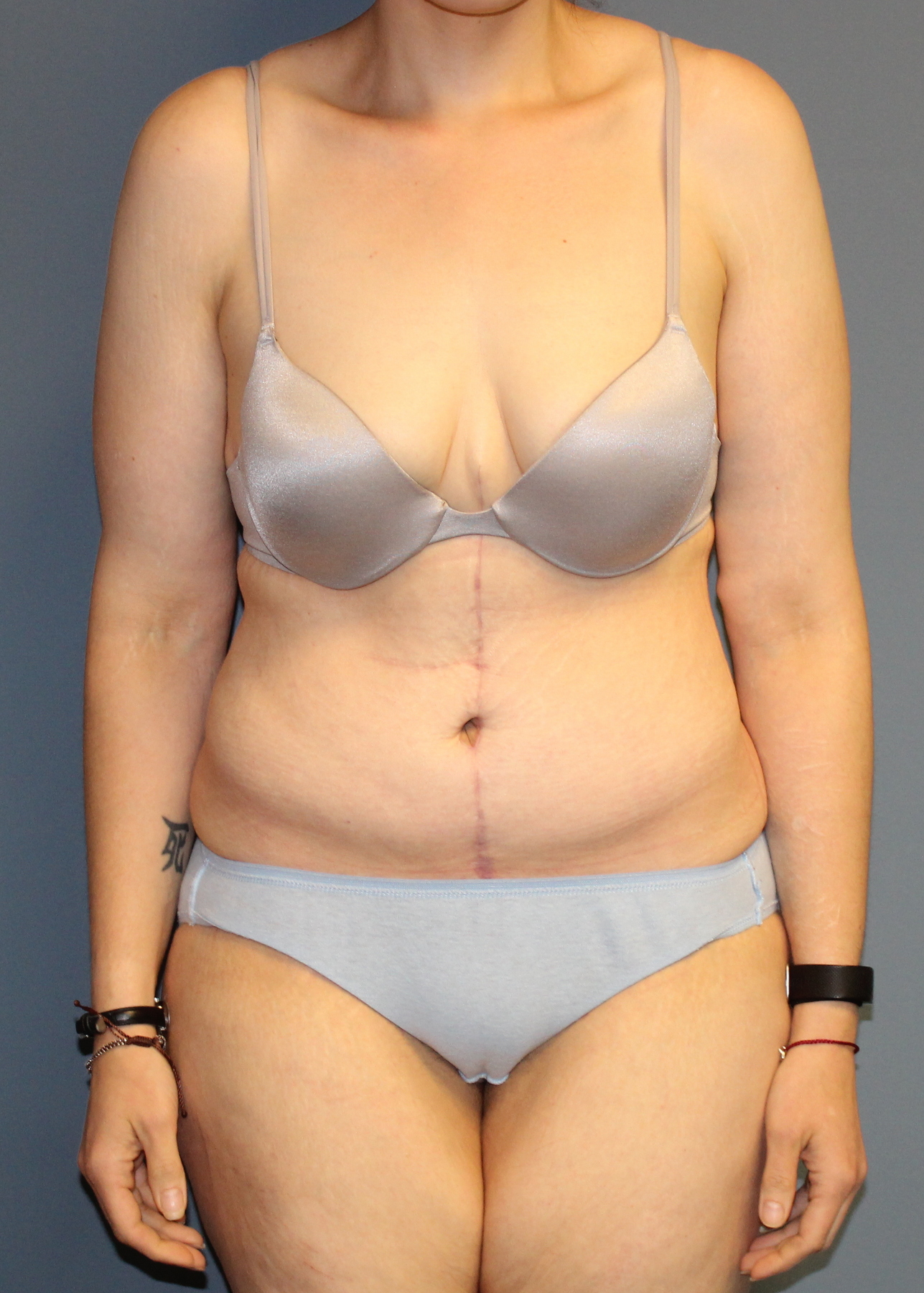
Corset Abdominoplasty
What is a Corset Abdominoplasty?
Not every discrete roll of fat is removed with a tummy tuck. The skin is not like an accordion where a pull flattens everything. Some patients have extra rolls in the upper abdomen. These rolls can be cut out later with a scar underneath the breasts (think of it as a reverse tummy tuck). If the skin removal goes all the way around the back, some would call that an upper body lift. I favor staging the upper part of the corset until after the Fleur-de-Lis has healed. When done at the same time, there can be a higher risk of healing issues due to diminished blood supply. The patient below had a staged Fleur-de-Lis tummy tuck and an upper body lift.
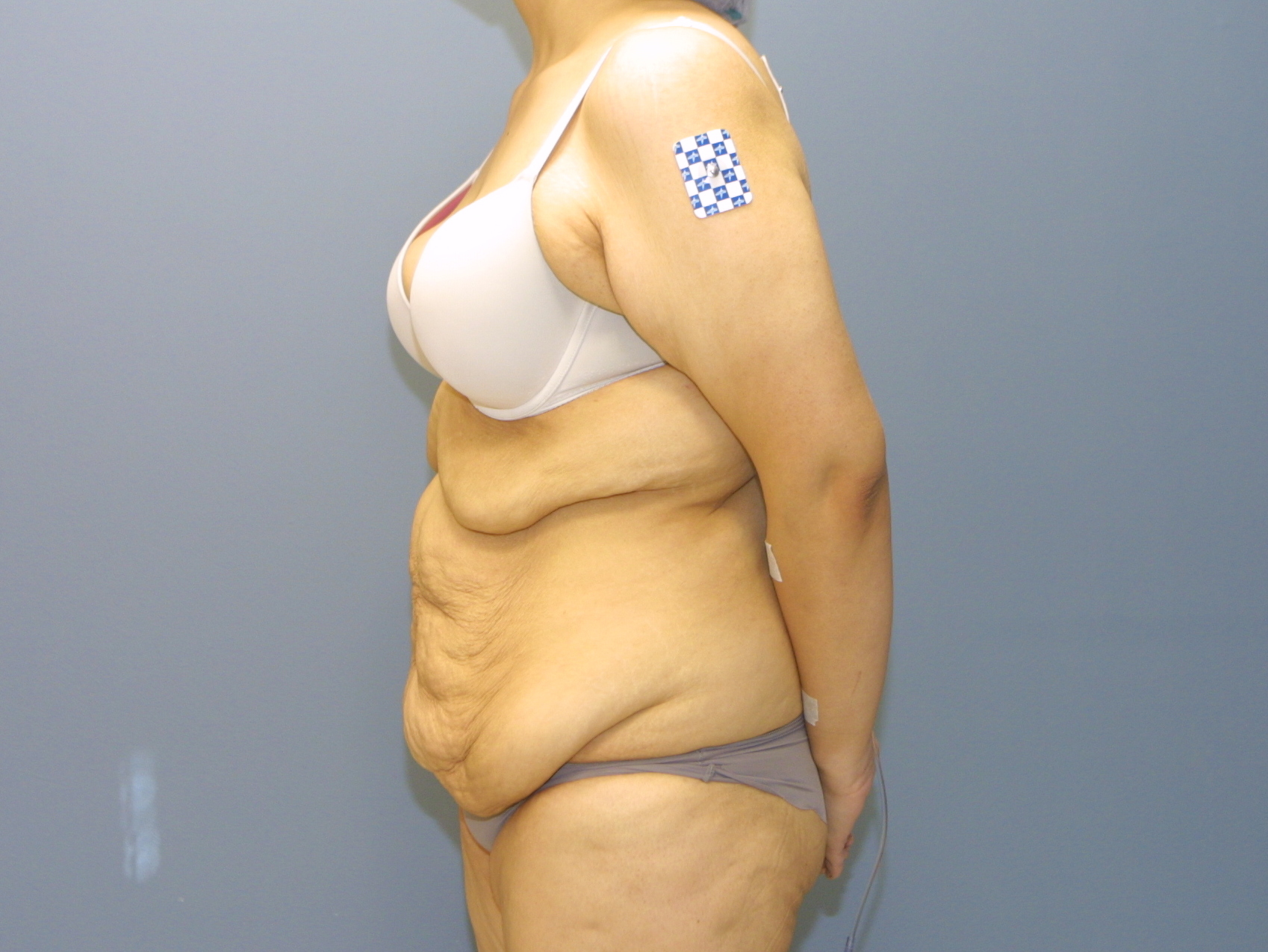{kind=link}
{kind=link}
Belt Lipectomy, or a 360 Degree Tummy Tuck (AKA, Body Lift)
I favor doing front first and if needed, stage the back to complete a 360 tummy tuck (also known as a belt lipectomy). When I do a standard or Fleur-de-Lis tummy tuck, I am pulling that patient forward (literally in the operating room) to remove as much vertical skin laxity as I can. If I were tightening the back at the same time, I would be pulling in the opposite direction and fighting my tummy tuck goals. When the tummy has healed and the patient can not only stand straight again, but also lie flat, then the patient will achieve a tighter abdomen as well as a tighter back. I can demonstrate this in an office visit.
While there are a few other tummy tuck variations, what I have discussed above are most relevant to the massive weight loss patient. More can be seen at www.DCtummytuck.com
Labia and pubis
The pubis often sags after massive weight loss, but this is what I call part of the win/win part of a tummy tuck. In a tummy tuck we pull loose skin down, but as a consequence the pubis is lifted up – win/win.
There is a little more to it than that. As a consequence of enlarging and deflating, just like in the abdomen, there is actually an excess of skin in the pubic mound. If I pulled it up it might reach as high as the belly button. To prevent this, I do a few things:
- I get rid of this extra skin by shortening the height of the pubic mound
- I will often thin the layer of fat under the pubic mound so it lines up with the level of the abdominal skin I have just pulled down
- I quilt the pubis and the abdomen. What does this mean? I sew the tummy down internally (like a quilt but inside only) so that the scar stays as low as possible and the skin we have pulled downwards heals more swiftly. The top of the pubic mound is also secured to this lower edge. It is an effort to keep the skin as low and tight as possible while preventing the pubis from coming up too high
When I discuss labia here in the weight loss patient it is usually the labia majora that have deflated somewhat. Redundant skin can be excised here as well. I have not found the labia minora to change excessively in weight loss, but if necessary, labia can certainly be reduced.
Thighs
While you will see a million photos of breast surgeries, tummy tucks, and other things on the internet, pictures of thigh lifts are far less common. Reason: they are far less gratifying. To put this in perspective, when a tummy tuck is performed we pull the tummy down and the loose pubis pulls up – this is pretty much a win/win as discussed above. Thighs are different. We pull them up and gravity wants to pull them back down, especially in the weight loss patient with lax skin. It doesn’t mean we can’t make improvement, patients just have to understand the limitations. I prefer the term “thigh tightening” as we do more skin tightening than actually lifting.
There are different types of thigh lifts depending on the degree of laxity.
Crescent Thigh Lift: An upwards pull in the groin and is fine for limited laxity specifically in that area. The incision is placed in the groin and buttocks crease.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
“L” or “Boomerang” Thigh Lift: My go to. It is a single incision that runs down the groin and continues to the inside of the leg towards the knee. The distance of the incision to the knee depends upon how much horizontal thigh laxity the patient has. This lift is both a vertical tightener and horizontal tightener of thigh skin laxity. Liposuction is used to thin the skin before removal in order to preserve lymphatic drainage of the lower leg.
Some patients may consider a staged excision of skin above the knee or a wedge of skin below the buttocks as well, areas that this lift does not address.
Because it is just one linear scar, this thigh lift has a lower chance to unexpectedly open due to motion after surgery. The patient below lost over a hundred pounds and has had a Fleur-de-Lis tummy tuck and an L thighplasty.
{kind=link}
{kind=link}
{kind=link}
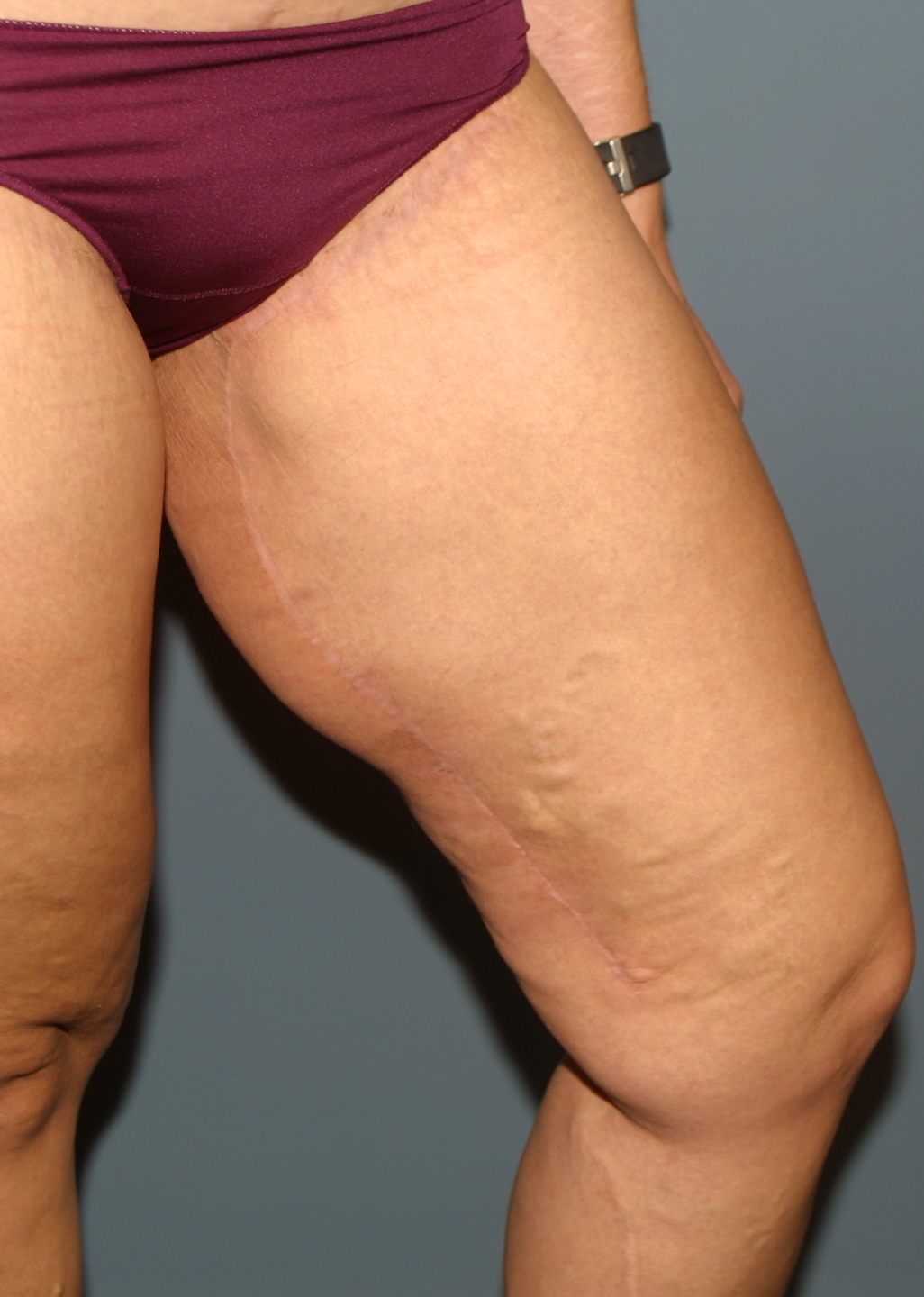{kind=link}
“T” Thighplasty: Combines a crescent thigh lift with a vertical incision inside the leg. If you read that section think of it as Fleur-de-Lis for your thigh.
Because it goes from front to back it can be more prone to opening under the buttocks, particularly when sitting. For this reason, I usually favor the L thigh lift and may stage the lower buttock incision if needed.
The patient below has had a T thighplasty.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
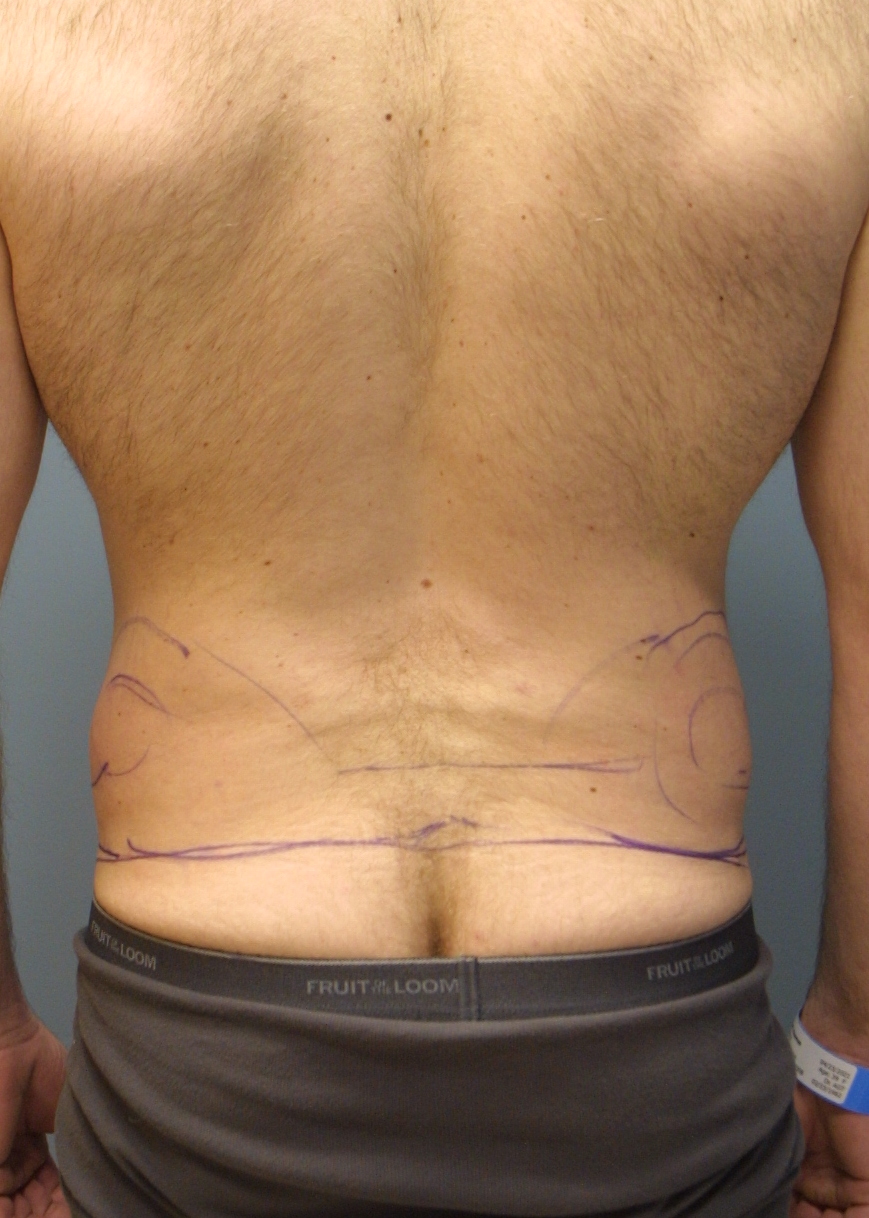
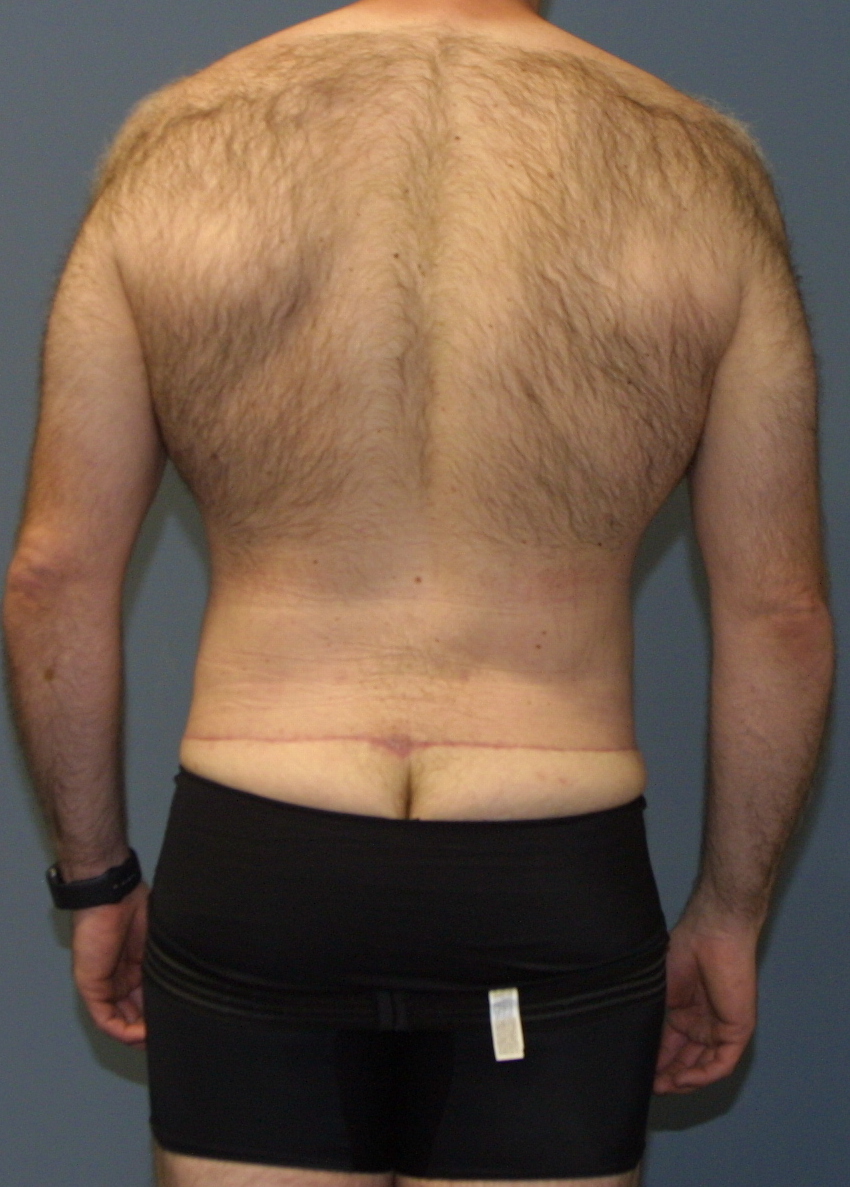
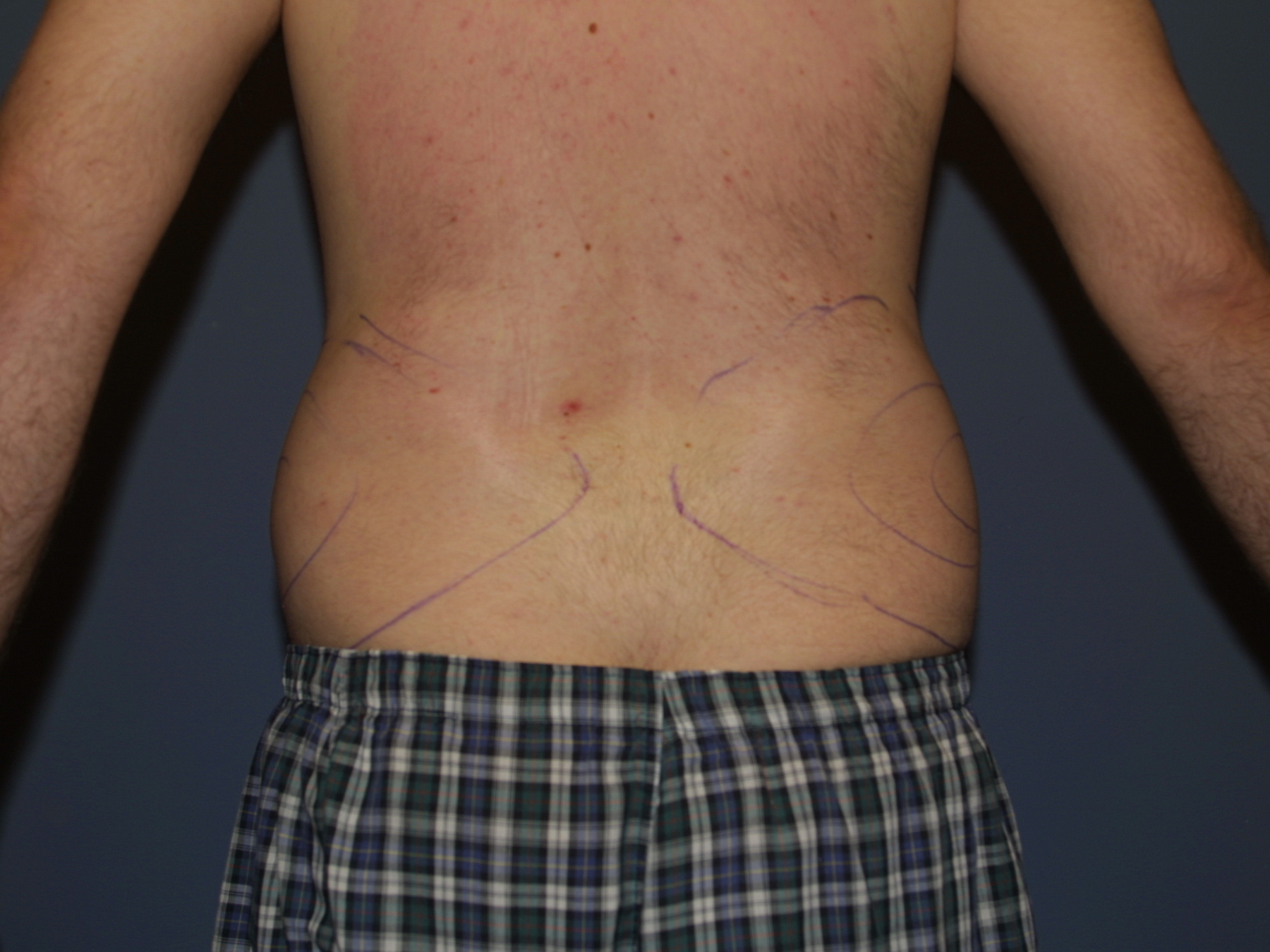
Back and flanks
It is very common for a weight loss patient to request liposuction of the back and flanks. For most though, it is a bad idea. Liposuction takes away the fat, but not the skin and what most of these patients have is loose skin. For most, the better answer is to remove the excess skin and fat combined. Alas, the back is not like the tummy. Because of the type of blood supply, the abdomen can be lifted like a sheet on your bed and tucked downwards. The back is different. It has what is called a segmental blood supply and if we lifted it up like a sheet, it would not survive. However, individual segments (remember segmental blood supply) can be safely removed. The most common excision is the bra strap excision (pictured below). This removes bulges in the upper back. Lower back excess can also be segmentally removed as staged procedures.
Upper Body Lift
{kind=link}
{kind=link}
Bra Strap Excision
{kind=link}
{kind=link}
{kind=link}
Lower Back Wedge Excision
{kind=link}
{kind=link}
What? No Lipo?
But Dr. T, You haven’t suggested any liposuction!!
As touched on above massive weight loss patients have loose skin. By the time they get to me they have often achieved 100 lbs or more of their own liposuction through diet and exercise, surgery or newer injectable drugs. It has left them loose and liposuction would make the problem worse. My weight loss patients are about skin tightening not loosening. Do not despair. For the right lump or bulge I am happy to bring out the liposuction cannula for conturing, but my first endeavor is to tighten. The patient below has good skin elasticity and has shrunk up nicely after liposuction.
{kind=link}
{kind=link}
Buttocks
Buttocks can be challenging in the massive weight loss patient. If the bum is still very heavy it will still want to sag. If it is deflated it can be hard to find fat to fill it in a patient who has already had massive weight loss. Buttocks must really be individualized. Sometimes a wedge of skin removed above or below the buttocks may improve contour. BBL can be considered if the skin envelope is tight enough and harvesting fat won’t deflate another area.
Example of Buttock Contouring with Fat Addition and Removal
{kind=link}
{kind=link}
{kind=link}
{kind=link}
My Personal road map
While each patient is different and not all procedures are appropriate, there is a very consistent path for many after weight loss.
Most patients start with breast and tummy surgery. These two are often combined because they are the most gratifying and often give the grandest changes. Because of patient positioning they are easy to combine.
Next:
Arm lift – if needed, usually done after a breast lift or reduction has healed.
Next:
Back wedges – If upper back I favor this after a breast lift or brachioplasty has healed.
If lower back/buttock lift I favor this after a completed tummy tuck has healed.
Next:
Facial rejuvenation – It is remarkable to me how even after massive weight loss many do not require facelift, but for those that do, often the starting points are the surgeries listed above.
Last:
Thigh lift – For the surgeries listed above risk of infection is never zero, but is generally quite low. A thigh lift lives in the groin near the vagina and rectum. For this reason the infection risk can be higher. Because of this higher risk I tend to favor thigh lift as an isolated procedure, often last.
Conclusion or "TLDR"
If you have read all the way to here that makes me very happy, but if not, don’t worry. A consult will hopefully make up the difference.
I love to teach, and I take pride in educating my patients about what can and can not be accomplished, what is real and what is wishful on the very dangerous internet. Which expectations are realistic and which are not.
I don’t always tell patients what they want to hear, but it is always my hope that when they leave my consultation, what I have taught makes sense, not just from my teaching, but independent intellectual sense. An informed patient is a better patient, a more realistic patient, a safer patient and ultimately, I hope, a happier patient.
I hope you have enjoyed this mini web site. Please feel free to contact me if you have any questions or comments.
Dr Tattelbaum's websites
About Dr. Adam Tattelbaum

The son of artist and a clergyman, Dr. Adam Tattelbaum grew up in a household where artistry and enhancing the lives of others took equal place. “I always knew that I wanted an occupation where I could work with my hands but also make a positive difference in people’s lives. I can think of no field in medicine that is more creative, gratifying or exciting.”
Born in New York City, Dr. Tattelbaum has performed plastic surgery in the Metropolitan Washington D.C. area for almost 30 years. Trained at Columbia, Harvard and Georgetown University, Dr. Tattelbaum is certified by both the American Board of Plastic Surgery and the American Board of Surgery. He is a member of the American Society of Plastic Surgeons as well as the American Society of Aesthetic Plastic Surgery which serves as a mark of distinction in cosmetic plastic surgery. He serves on the clinical faculty at Georgetown University, where he has taught. Listed on multiple occasions as a Washingtonian and Bethesda Magazine Top Doctor, his greatest joy is the teaching and education of his patients. He offers a common sense approach to cosmetic surgery and offers the same advice to patients that he would offer to his family and friends.
Husband and proud father of two, Dr. Tattelbaum and his wife live in Maryland.